Niger J Paed 2014; 41 (4): 295 - 301
ORIGINAL
Umar LW
Successes and challenges of
Osinusi K
under-five child mortality
reduction in West Africa
DOI:http://dx.doi.org/10.4314/njp.v41i4,1
Accepted: 10th May 2014
Abstract
Background: Under-five
tions still remain the leading
mortality rate is an important in-
causes of death. In spite of a five-
Umar LW
(
)
dex
for assessing achievements by
fold rise of average annual rate of
Department of Paediatrics
countries and thus its targeted
reduction of under-five deaths
Ahmadu Bello University Teaching
reduction is adopted as bench-
compared to a 3-fold rise of the
Hospital Shika-Zaria
mark towards realizing the Mil-
global average and a 49.7% reduc-
Email: umarlw@gmail.com
lennium Development Goal num-
tion in under-five mortality rate,
Osinusi K
ber 4 by 2015. With less than 24
the sub-region trails behind other
Department of Paediatrics,
months to the deadline, West Af-
parts of Africa. While only Liberia
UCH
Ibadan
rica still contributes significantly
achieved the MDG 4 target, Niger,
to
the global burden of child mor-
Cape Verde, Gambia, Guinea and
tality, with over half of the deaths
Burkina Faso are on track. Nige-
caused by infections.
ria’s huge child population, high
Objective: To
review the
suc-
under-five mortality burden and
cesses and challenges of reducing
slow reduction, weighs down the
under-five mortality in West Af-
sub-region’s averages. Neonatal
rica.
death proportions are rising, with
Sources: A
search was
made in
four countries ranking amongst the
Pub Med and Google Scholar
world’s top ten. With less than 24
using the key words: Under-five,
months left, the likelihood of
Children, Mortality, West Africa,
achieving the reduction targets for
Successes,
Progress,
Achieve-
under-five mortality in most of the
ments and Challenges .
Relevant
countries in the sub-region by the
publications and reports available
end of 2015 remains a mirage.
at
WHO, UNICEF and UN web-
Conclusion: Numerous
daunting
sites were also consulted. Tables
challenges have contributed to
and charts were drawn from rele-
slow the pace of under-five death
vant data for West African Coun-
reduction in West Africa. Coun-
tries obtained from these sources
tries in the sub-region need to ad-
using Microsoft® Excel® for
dress their challenges while scal-
Mac
2011
Version
14.1.0
ing
up proven interventions to ac-
(110310).
celerate progress towards further
Results: Although
significant un-
reductions of under-five deaths.
der-five death reductions have
been recorded in countries of
Key words:
Children,
under-five,
West Africa between 1990 and
mortality, West Africa, progress,
2012, the reduction falls far short
successes, achievements,
of
the expected targets and infec-
challenges
Introduction
and achievement of 90% measles immunization cover-
age for children 12-24 months of age by the year 2015 .
1
At
the Millennium Development Summit in September
Other health-related MDGs are one (eradicating poverty
2000, world leaders and development experts made the
and hunger), five (improvement of maternal health), six
famous declaration that committed the global commu-
(combating HIV, malaria and TB), seven (environmental
nity to the eight Millennium Development Goals
sustainability) and eight (forging global partnerships).
(MDGs) to address poverty, hunger, diseases and envi-
The
fifteen countries in West Africa cover a vast ex-
ronmental degradation. The MDG 4 seeks to improve
panse of landmass extending from Senegal in the north-
survival of children by reducing under-five mortality
east, to the Gulf of Guinea, the Lake Chad and the high-
aiming at three benchmarks: reduction of under-five and
lands bordering Nigeria and Cameroon to the west. The
infant mortality rates by two-thirds of the 1990 figures
average total population in 2011 was about 316 million
296
with a range from 0.5 million in Cape Verde to 160 mil-
Successes in Under-Five Mortality Reduction
lion in Nigeria. Under-5 child proportions range from
Global ranking
10.3% to 19.9% (average of 16.3) and Nigeria has the
highest under-5 population of nearly 27.2 million, or
There has been a significant reduction of under-five
50.2% of the total in the sub-region .
2
mortality among West African countries from 1990
The
countries belong to the “Lower Income” and
when eight countries had mortality rates above
“Lower
Middle Income” groups with the
lowest GDP
200/1,000 live births, while the rest had rates above
per Capita range of $290 in Liberia to $2940 in Cape
100/1,000 live births. By the end of 2012 none has a rate
Verde, and half of citizens in eight countries living on
above 200/1,000 live births while seven had rates of less
than 100/1,000 live birth . The sub-region however,
4,5
less than $1/day . All are also among the group of “75
2
Countdown” countries sharing over 95% of the global
still remains home to eight of the top fifteen in the
maternal and child deaths .
3
global ranking of under-5 mortality (Table 1).
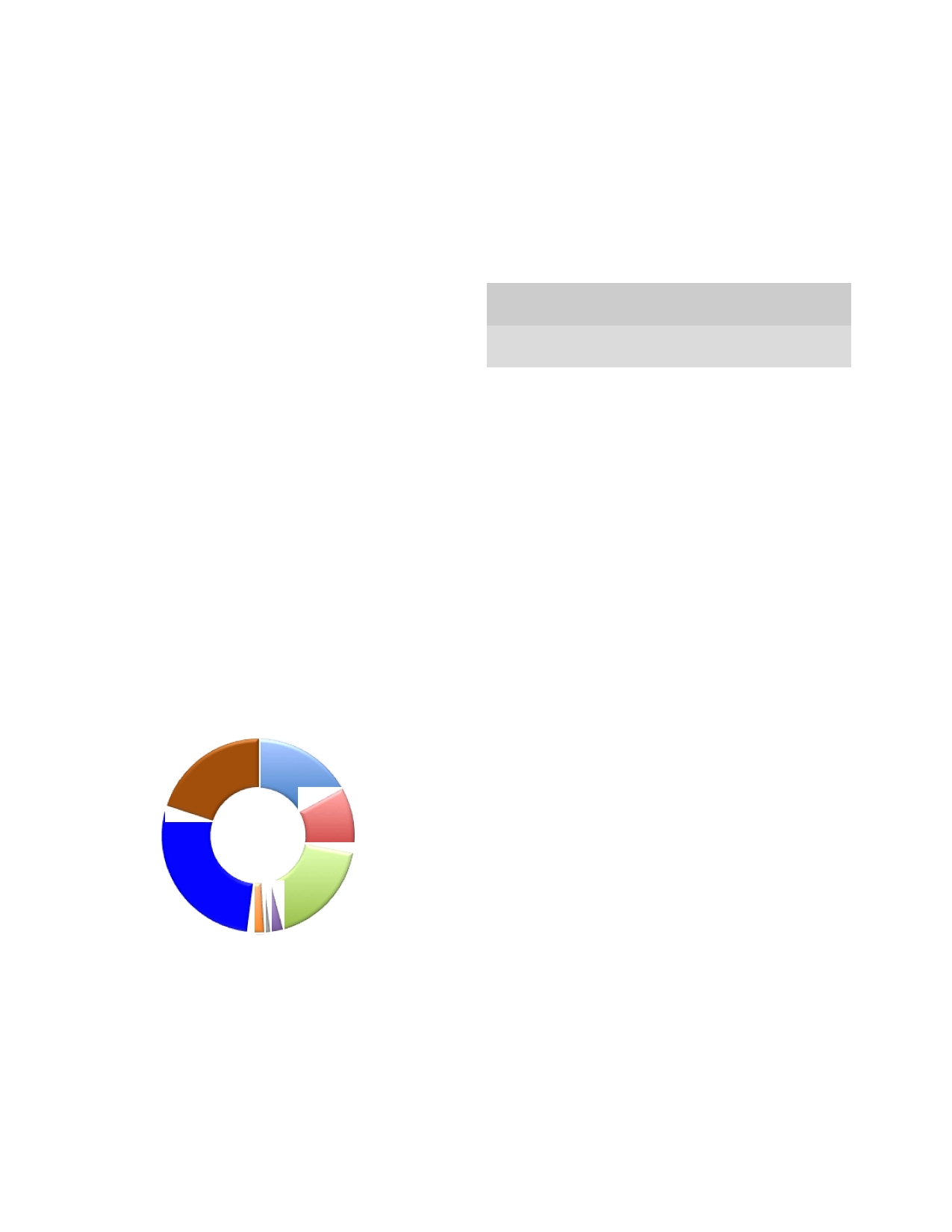
Major causes of child mortality
Table 1: Global
ranking of
under-5 mortality
rates (per
1000
live births) for West Africa, 2012
Infectious diseases have remained the major cause of
%
Reduc-
deaths in children in the sub-region (Figure 1). For in-
U5MR
U5MR
tion from
U5MR
*AAR
Country
1990
2012
1990
Rank
R(%)
stance, amongst fifteen countries with the highest bur-
den
of deaths due to pneumonia and diarrhoea, countries
Sierra Leone
257
182
29
1
1.6
Guinea-
in
the sub-region had 23% of the 1.3 million deaths
Bissau
206
129
37
6
2.1
shared by these countries by the end of 2012 . Nigeria
4,5
Mali
253
128
49
8
3.1
alone has 18% while Niger, Mali and Burkina Faso,
Nigeria
213
124
42
9
2.5
share 5%. Morbidity and mortality due to malaria have
Niger
326
114
65
10
4.8
become largely concentrated in countries of West and
Côte d'Ivoire
152
108
29
11
1.6
Central Africa, together being responsible for 65% of
Burkina Faso
202
102
49
14
3.1
the mortality burden for the top 10 countries or 3.1 mil-
Guinea
241
101
58
15
3.9
lion deaths. Nigeria alone has 46% of this figure while
Togo
143
96
33
19
1.8
Benin
181
90
50
22
3.2
Mali, Cote d’Ivoire, Niger and Burkina Faso together
Liberia
248
75
70
32
5.4
share 19% . Neonatal problems account for 28% of all
4,5
Gambia
170
73
57
33
3.8
under-five deaths, with birth asphyxia and prematurity
Ghana
128
72
44
36
2.6
causing 57% while neonatal sepsis, pneumonia and
Senegal
142
60
58
43
3.9
meningitis together cause 25%. Countries of West
Cape
Verde
62
22
64
88
4.6
Africa that feature prominently among top ten countries
with highest neonatal death rates include Cote d’Ivoire,
*AARR: Average Annual Rate of Reduction of under-5 mortality
Guinea Bissau, Mali and Sierra Leone .
4
Major contribution to under-five mortality decline
Fig 1: Major
causes of
under-five mortality in
West Africa,
2012
The Major decline in deaths was from reduction of
deaths due to infectious diseases, of which measles
Pneumonia,
17%
deaths reduction by over 80% was the most remarkable.
Others,
20%
The average measles immunization coverage in the sub-
region is however yet to reach the 90% target for
MDG4, improving from an average of 58% to 79% and
Diarrhoea,
11%
only five countries reached the 2015 target of 90% by
end of 2012 .
4
Neonatal,
28%
The 2013 UNICEF MDG Report revealed that based on
Malaria,
18%
regional group analysis West and Central Africa
achieved average reductions of 23% for neonatal mortal-
HIV,
2%
ity, 33% for infant mortality and 39% for under-five
Injuries,
3%
Measles,
1%
mortality from the 1990 rates . When analyzed sepa-
4
HIV/AIDS is responsible for 1-4% of deaths across the
rately however, West Africa’s progress still fall short of
the 2/3 MDG4 reduction targets, with average reduc-
rd
countries in the sub-region, and out of the total global
under-five deaths of about 103,000 due to the disease in
tion of 30.4% for neonatal mortality, 42.7% for infant
2012, Nigeria has the highest of 24,000 or 23%. At the
4
mortality and 49.7%, for under-five mortality between
sub-regional level this burden far outweighs the sum for
1990 and 2013.
other countries put together while at the global level
Nigeria remains the country with the second lowest anti-
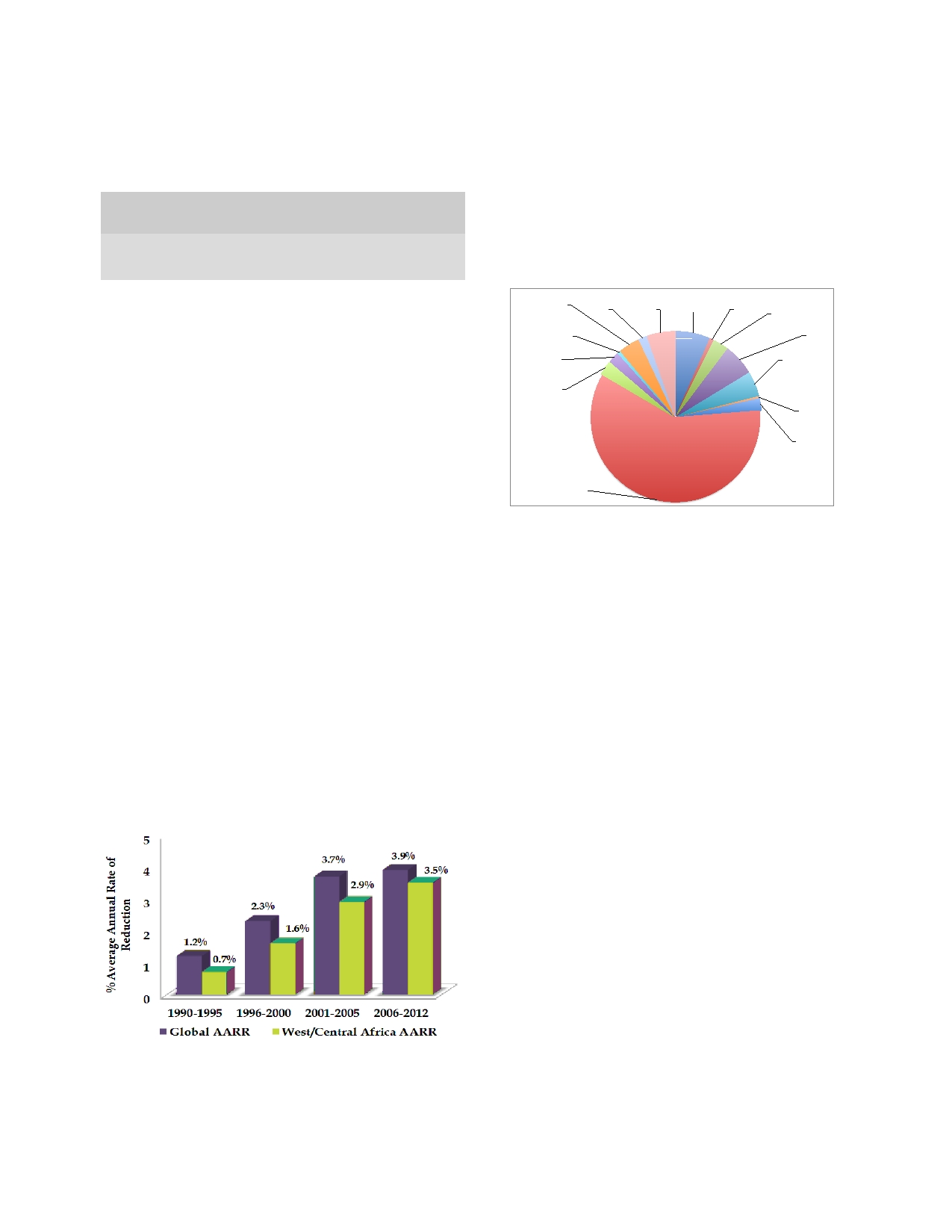
Absolute Progress
retroviral therapy coverage for eligible children (12%)
out of the 22 countries with the highest burden of HIV
The MDGs have been argued to be too ambitious for sub
infection. The average prevalence of stunting in West
-Saharan Africa because although they were set in 2000,
Africa is about 40% and under-nutrition is associated
their monitoring was backdated to begin from 1990.
with up to a third of under-five deaths in the sub-region .
4
This makes progress difficult for these countries since
297
they
had poor development indices in the 1990s and
mortality burden, with Nigeria alone responsible for
were
confronted by numerous challenges along the line.
827,000 deaths or 13% as at the end of 2013, coming
While the MDG4 measures relative progress or extent of
second to India’s 22%. At the sub-regional level 60% of
death reduction from 1990, absolute progress measures
the
burden lies with Nigeria alone, while each of the
the
total change made. West African countries fared
other countries have less than 10% of the total under-
five mortality as at the end of 2012 (Figure 3) .
4
better by absolute progress ranking than by relative
ranking (Table 2)
6,7,8,9,10
.
With a 2011 population of 162 million, Nigeria’s under-
five
population of about 27.2 million is over half the
Table 2: Under-five
mortality (U5MR)
global absolute
and
region’s under-five population , partly accounting for its
2
relative ranking for West African countries, 1990-2007*
relatively higher burden.
Absolute
Relative
U5MR
U5MR
Progress
Progress
Fig 3: Under-five
mortality burden
in West
Africa, 2012
(% of
Country
1990
2007
Rank
Rank
1.5
million)
Niger
304
176
1
60
Togo
Cote
d’Ivoire
Niger
Liberia
Guinea
231
150
9
73
Ghana
2%
5%
1%
4%
6%
Guinea
Liberia
205
133
13
72
3%
Mali
Benin
184
123
16
77
Guinea-Bissau
6%
1%
Mali
250
196
26
100
Senegal
Burkina
Faso
Togo
150
100
30
75
2%
5%
Gambia
153
109
37
89
Cape
Verde
Guinea-Bissau
240
198
39
106
Sierra
Leone
3%
0%
Nigeria
230
189
41
104
Gambia
Senegal
149
114
50
97
0%
Cape
Verde
60
32
61
41
Benin
Sierra Leone
290
262
61
113
2%
Côte d'Ivoire
151
127
71
109
Burkina Faso
206
191
89
116
Ghana
120
115
113
121
Nigeria
60%
* Modified from:
Overseas Development Institute, 2010. The Millennium Development
Countries with the Most Impressive Progress
Goals Report Card. Measuring Progress Across Countries. September
2010
The countries with the most impressive under-five mor-
The 2013 UNICEF MDG Report that included analysis
tality decline were Niger and Liberia with average an-
of
United Nation’s Inter-agency Group for Child Mor-
nual
rate of reduction (AARR) of 4.8% and 5.4% and
tality Estimation (IGME) data demonstrated the faster
reductions of 65% and 70% from the 1990 rates respec-
tively . These lower income countries successfully
4
rate of under-five mortality reduction in West and Cen-
tral Africa by absolute average rate of reduction from
scaled up major interventions that improved universal
1990 to 2012 compared to the global average (Figure 2).
access for the leading killer diseases of children includ-
These sub-regions recorded a five times rise in average
ing malaria, pneumonia, diarrhoea, malnutrition and
HIV
2,3,4,5,11
annual rate of reduction (AARR) compared to only a
.
tripling of the global average in the period 1990 to
In
Niger 22% of under-five death reductions were attrib-
2012 .
4,5
uted to improved care-seeking for pneumonia and diar-
rhoea, 25% due to provision of insecticide treated mos-
Fig 2: West/Central
Africa’s Rise
of Under-5
Mortality
quito nets (ITN) to under-five children and 19% to nutri-
tion intervention programmes
11,12,13
Reduction*
.
In Liberia by the
end of 2010 ITN provision for under-five children was
raised to 73% thereby halving malaria prevalence,
prevalence of severe malnutrition fell to 2.2% due to
enrolment of 50% of severely malnourished children in
a basic
care package, PMTCT and ART
coverage have
improved to 69% of eligible women and to 44% of eligi-
ble children while neonatal tetanus has also been elimi-
11,12,14
nated by the end of 2010
.
Nigeria’s under-five mortality burden
Nigeria’s performance in under-five death reduction
apparently weighs down both West Africa’s and sub-
*Modified
from:
Saharan Africa’s averages, with a population of about
4.
United Nations Children’s Fund, New York (2013). Committing to
51.4% of West Africa’s total as at 2011. While Nigeria’s
Child Survival: A Promise Renewed: Progress Report 2013. Accessed
15
September 2013. Available at, www.apromiserenewed.org.
under-five population of 27.2 million is equivalent to
about half (51.6%) of the total under-five population in
In
spite of these achievements West African countries
the sub-region, its under-five mortality proportion of
remain prominent in the global league for under-five
60% by the end of 2012 is disproportionately higher
than the country’s contribution to the total under-five

298
population in the sub-region . The country had a 1990
2
half
of children with suspected pneumonia are taken to a
under-five mortality rate of 213/1,000 live births an
health care provider and there is sub-optimal use of anti-
AARR of 2.0% and its total reduction of 42% from the
biotics among those attended to. Similarly there is poor
1990 rate is amongst the six lowest in the sub-region.
4
utilization of oral rehydration salts (ORS) and zinc for
Nigeria’s rapid population growth is faster than the pace
children in Nigeria, Mali and Niger that have the highest
of
scale-up of services. For instance, as the annual num-
diarrhoeal disease burden and deaths in the sub-
region
11,12
ber of births rose from 4.3 million to 6.1 million be-
.
tween 1990 and 2008 and the number of births attended
to
by skilled providers doubled from 1.3 million to 2.7
Sub-optimal routine immunization
million, the service coverage rose by only 8% (31% to
39%). Had the number of births remained stable the cov-
While routine immunizations coverage improved in Li-
erage could have reached 63%, much higher than the 8%
beria and Niger, sub-optimal routine immunization cov-
rise
2,3,17
.
erage and inconsistent immunization campaigns in some
parts of Nigeria have contributed to resurgence of out-
breaks of measles . Meanwhile the global annual bur-
16
The Challenges of Reducing Under-five Mortality in
West Africa
den of measles was reported by WHO to have reduced
from 853,500 cases in 2000 to 355,000 cases in 2011
Several challenges have contributed to slow down the
with a decline of mortality globally by 71% between
2000 and 2011, from 542 000 to 158 000 deaths.
26,
27
progress of West African countries towards reduction of
under-five deaths, many of which are common to all the
The WHO has estimated that about 1.7 million out of
countries while a few are unique to each country. Fore-
the 20 million unprotected children live in Nigeria with
most among the common challenges are:
up
to 18,843 cases reported in measles outbreaks in the
country in 2011 alone .
26
Funding constraints
Human resource constraints
Both domestic and external funding (MDG 8 targets) for
the implementation of MDG interventions are falling
The sub-region has the severest shortage of health care
short of expectation. For instance funding from the
personnel with a density of less than two health workers
Overseas Development Assistance (ODA), which com-
per 1,000 persons, much lower than the WHO standard
mits developed countries to set aside 0.7% of their Gross
of
2.3 per 1,000. Health care workers are much fewer in
National Income (GNI) towards MDG funding has been
rural, remote and hard to reach areas and where avail-
dwindling especially due to the global economic crisis in
able, they often have inappropriate skill mix, performing
jobs not suited for their competencies
17,18,19
the last decade. Similarly, commitments made by Afri-
.
can
leaders in the“2001
Abuja Declaration” were
not
being fulfilled, with only five of the countries in the sub-
Inadequate water supply and poor environmental sani-
region keeping their promise of setting aside 15% of
tation
their national budgets for health as at 2011
15,20
.
There is generally poor access to safe potable water re-
Poverty, hunger, malnutrition and poor maternal educa-
sulting in high diarrhoeal disease prevalence and higher
tion
burden of diarrhoeal disease mortality. There is gener-
ally slow progress in realizing the environmental sus-
West African countries are among those with the highest
tainability targets (MDG 7) in most countries in the sub-
under-five death rates in the poorest households. Mortal-
region, with less than 50% of citizens having access to
ity analysis by household wealth quintiles has revealed
supply of safe water. There is also poor environmental
that under-five children of the poorest 20% of house-
sanitation with the effect of contamination of surface
water
4,25
holds have at least a two-fold risk of mortality than
.
those in the richest quintile . There is also a three times
19
higher risk of under-five mortality in children of unedu-
High out of pocket expenses for health
cated mothers compared to those of mothers that had
secondary level of education . Countries like Niger,
19
The
countries in West Africa generally have high out of
Mali
and Guinea Bissau have serious to alarming levels
pocket expenses for health from family income for their
of
hunger as rated on the Global Hunger
Index. The
citizens. For instance these expenses make up above
lingering poverty coupled with food insecurity is aggra-
50%
in half of the countries and is up to 88% in Guinea
vated by adverse climatic changes, as well as civil un-
and
94% in Cape Verde. The Governments’ per capita
rest, all of which have contributed to high rates of mal-
expenditure on health is also quite low, being less than
15%
across the sub-region .
2,6
nutrition and increased vulnerability of children to infec-
tions
11,12
.
Slow rate of maternal mortality reduction
Poor utilization of health services
Maternal mortality ratio ranks amongst the highest in the
There is generally poor health seeking behaviour for
world due to poor progress in reduction of peripartum
children across the sub-region. For instance, less than
deaths across the sub-region. Nigeria has one of the
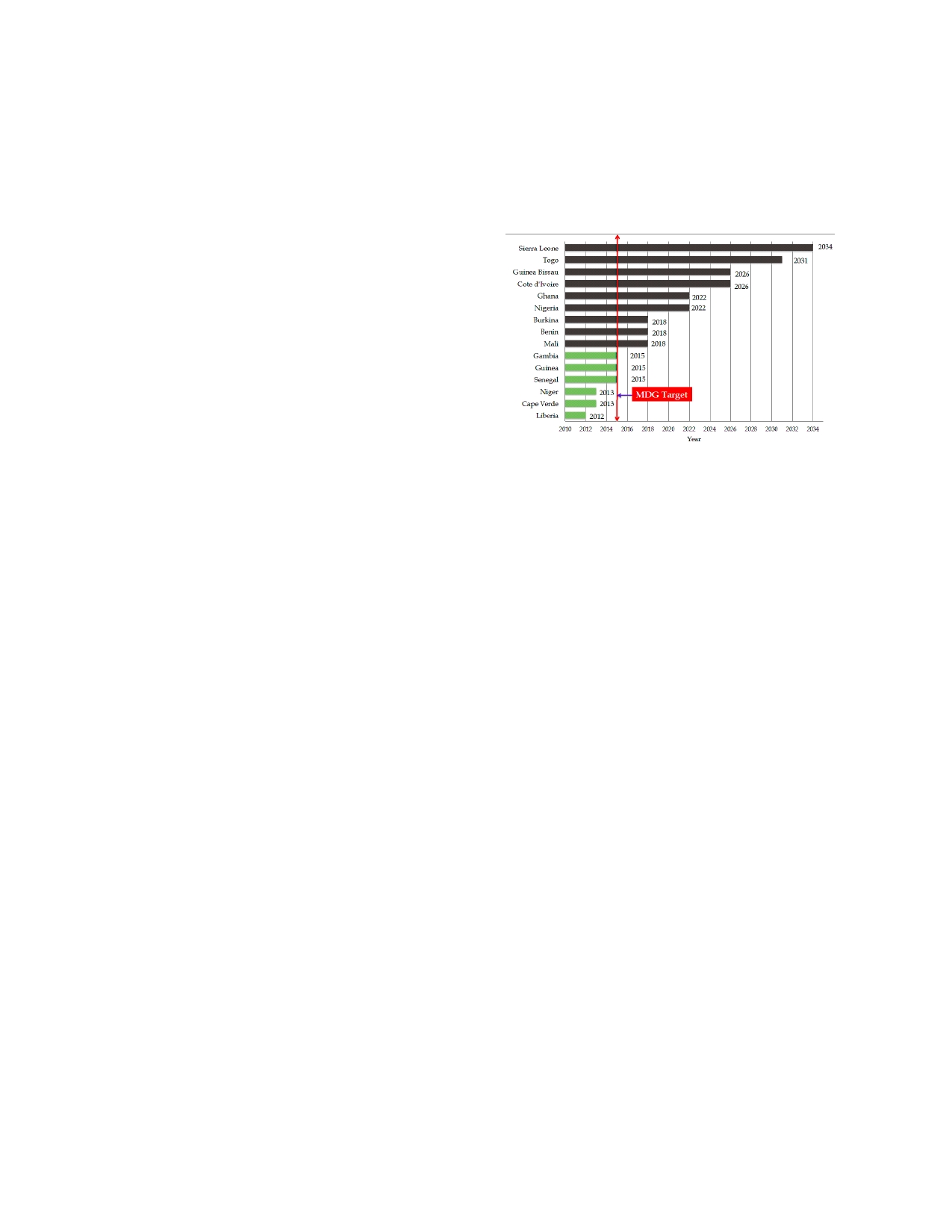
299
highest maternal mortality rates in the sub-region, with a
able
to reduce their under-five mortality to the expected
level till up to two decades after 2015 (Figure 4) . As a
4
national average of 545/100,000 live births and nearly
twice this in the north east and north west zones
sub-region therefore, even though West Africa has re-
(1000/100,000). Maternal deaths consequently increases
corded undisputed successes in child death reductions
vulnerability of orphans, further predisposing them to
over
the last decade, it is unlikely to achieve the desired
inadequate care and malnutrition, with negative impact
global benchmark for under-five morality reductions in
on
their chances of survival
3,4,19
.
the
remaining period to the end of 2015.
Slow rate of neonatal mortality reduction
Fig 4: Year
at which
West African
Countries would
Achieve
MDG4
Reduction of neonatal deaths lags behind under-5 mor-
tality decline as a result of which the average share
among total under-5 deaths rose from 36% to 40% from
1990. The absolute number of neonatal deaths rose
above the 1990 figures in some countries like Nigeria
3,4,5
.
A large proportion of neonatal deaths are attribut-
able to birth asphyxia following high rates of home de-
liveries that are often unsupervised by skilled attendants.
Rapid population growth
West African countries have about the highest popula-
tion growth rates constituting a huge challenge for ade-
quacy of health service coverage. The rate of population
Some development experts have disputed the current
growth is faster than the rate of scale up of services as
methodology for the measurement of success in achiev-
typified by Nigeria where there was marginal increase in
ing reduction of under-five mortality, proposing that
births attended by skilled personnel despite a two-fold
measurement is more objective when made by assessing
increase in number of skilled birth attendants over the
for pace of progress than by achievement of fixed tar-
gets . The official reports of the UNDP, World Bank,
10
period from 1990 to 2008
2,3,17
.
UNICEF and other UN agencies on successes of MDGs
Armed conflicts
placed much emphasis on achieving set targets and these
have portrayed sub-Saharan Africa as either being “off-
Most
countries of the sub-region have had their share of
track”, “missing the target” or having a “grossly insuffi-
one
type of conflict or another ranging from civil wars
cient rate of reduction”. It is further argued that as per-
and
sectarian/ethnic clashes to military take-over of
formance measures, MDG success should equally focus
power in coup d’états, which has disrupted equitable
on
pace or acceleration of progress relative to pre-2000
period rather than achieving projected targets . They
10
service delivery. Civil wars were fought in Sierra Leone,
Liberia, Guinea-Bissau and Cote d’Ivoire, Coups d’états
further observed that the current reported MDG achieve-
occurred in Gambia, Niger and Guinea while ethnic and
ments do not differentiate between background non-
sectarian clashes occurred frequently in Nigeria, Mali,
MDG
country
developmental
performance
from
Benin since 1990. These have caused displacement of
achievements solely attributed to MDG efforts, and so
populations and movements of people across borders
any
observed progress could as well have been at least
leading to vulnerable refugee settlements where child
partly as a result of efforts unrelated to MDG. In this
malnutrition and infectious disease incidence contribute
context, a proposed alternative method of analysis of
data from the period preceding 1990 , revealed empiri-
10
to
increased morbidity and mortality especially amongst
under-five children .
4
cal
findings suggesting that Africa’s MDG progress is
even faster than the global average , Other findings in
10
The Outlook for Reduction of Under-five Mortality
this regard include:
in West Africa
1.
A
63% acceleration (post-2000) of Africa’s under-5
With less than 24 months to the end of 2015, up to nine
mortality reduction against a global average of 32%.
countries including the most populous are unlikely to
2.
Nigeria, Burkina Faso and Senegal emerged among
achieve significant under-five death reductions, and
the world’s top 10 for under-5 mortality reduction
therefore may not be able to reach their 2/3 reduction
rd
and among the top 15 improvers of reduction by
targets at their current average annual rates of under-five
absolute pace of improvement.
mortality reduction (AARR). Although up till the end of
3.
When rated by AARR and comparing progress from
2013 only Liberia has attained the 2/3 under-5 mortal-
rd
1970 to 2010, 75% of sub-Saharan Africa had ac-
ity reduction from the 1990 rate, but with sustained pro-
celerated its AARR in the period between 2001 and
2010 over previous rates .
10
gress at the current AARR of 3.8-4.8% Niger, Cape
Verde, Senegal, Guinea and Gambia are likely to attain
their two-thirds reduction targets. At their current
Recommendations for the Way Forward
AARR counties like Togo and Sierra Leone may not be
With obscure prospects for achieving global reduction
300
goals and targets, West African countries need to focus
Conclusion
on
strategies to further accelerate their progress beyond
just
a focus on 2015 targets, specifically to:
West
Africa continues to have a huge burden of under-
1.
Improve political will and commitment to adopt and
five mortality in spite of considerable successes that
implement innovative health policies, strategies and
were
achieved by absolute progress a disadvantaged
interventions
4,19,21,23
.
status in 1990 and daunting challenges along the line.
2.
Review terms of development partnerships with
By
the current MDG benchmarks, realizing the two-
stakeholders through country-led selection of needs,
thirds under-5 mortality reduction target is unlikely for
taking the lead in setting their own national goals
West Africa. Countries in the sub-region would need to
and targets and channeling partner support towards
further strengthen and scale up successful strategies and
the
most essential interventions .
9
interventions, address the challenges, and take more
3.
Implement strategies to further address poverty alle-
ownership and responsibility towards combating
viation and reduce family out-of-pocket expenses
infectious diseases and neonatal deaths.
for
health
4,19
.
4.
Increase universal access to basic services and sup-
plies (drugs, vaccines) and rehabilitate physical
Conflict of interest: None
infrastructure by increase in budgets for the health
Funding: None
sector
13,14,15,20
.
5.
Accelerate efforts to address human resource gaps
through task shifting, mentoring and deployment of
skilled personnel to under served areas
3,4,11,17
.
References
1.
United Nations General Assembly
8.
Michael C, Moss T, Kenny C. The
15.
World Health Organization Ge-
New
York, 2000. The United Na-
Trouble with the MDGs: Confront-
neva, 2011. The Abuja Declara-
tions Millennium Declaration.
ing
Expectations of Aid and De-
tion: Ten Years On – 2001 Prom-
Eighth
plenary meeting. Septem-
velopment
Success. Washington
ises of commitment and solidarity.
ber
2000.
DC,
Centre for Global Develop-
Available at: http://www.who.int/
2.
World Health Organization Ge-
ment. 2004; CGD Working Paper
healthsystems/publications/
neva, 2013. World Health Statis-
40.
abuja_report_aug_2011.pdf.
tics 2013. ISBN 978 92 4 156458
9.
Vandemoortele J. Advancing the
16.
Weldegebriel GG, Gasasira A,
8.
Available at: http://
global development agenda post-
Harvey P, Masresha B, Goodson
health_statistics/en/
2015: Some thoughts, ideas and
JL,
Pate MA, et al. Measles resur-
index.html.www.who.int/gho/
practical suggestions. New York:
gence following a nationwide mea-
publications/world_
United Nations System Task Team
sles vaccination campaign in Nige-
3.
United Nations Children’s Fund
on
the Post-2015 United Nations
ria, 2005–2008. J
Infect Dis
2011;
New
York, 2012. Countdown to
Development Agenda 2012.
204 (1): S226–31.
2015. Building a Future for
10.
Fukuda-Parr S, Greenstein JP,
17.
World Health Organization Ge-
Women and Children: Maternal,
Stewart D. How should MDG
neva, 2011. Global Health Work-
Newborn and Child Survival, The
success and failure be judged:
force Statistics 2011 Update; avail-
2012 Report.
Faster progress or achieving the
able at: http://apps.who.int/
4.
United Nations Children’s Fund,
targets? World
Dev 2013;
41: 19-
globalatlas.
New
York (2013). Committing to
30.
18.
Blencowe H, Cousens S, Oester-
Child Survival: A Promise Re-
11.
Gill CJ, Young M, Schroder K, et
gaard M, Chou D, Moller AB, et
newed: Progress Report 2013.
al.
Bottlenecks, barriers, and solu-
al.
National, regional and world-
Accessed 15 September 2013.
tions: results from multi-country
wide estimates of preterm birth
Available at:
consultations focused on reduction
rates in the year 2010 with time
www.apromiserenewed.org.
of
childhood pneumonia and diar-
trends for selected countries since
5.
United Nations Children’s Fund
rhoea deaths. Lancet
2013; 381:
1990: a systematic analysis. 2012;
New
York, 2013. Levels and
1487-98.
CHERG/WHO.
Trends in Child Mortality: 2013
12.
United Nations Children's Fund
19.
United Nations Children’s Fund
Report. The UN Inter-agency
New
York, 2013. Improving Child
New
York, 2012. Committing to
Group for Child Mortality Estima-
Malnutrition: The achievable im-
child survival: a promise renewed:
tion (IGME).
perative for global progress.
Progress Report, 2012. Accessed
6.
Overseas Development Institute,
13.
Amouzou A, Habi O, Bensaid K.
13
September 2013. Available at:
2010. The Millennium Develop-
Reduction in child mortality in
http://www.apromiserenewed.org.
ment Goals Report Card. Measur-
Niger: a Countdown to 2015 coun-
20.
United Nations, New York, 2008.
ing
Progress Across Countries.
try
case study. Lancet
2012; 380:
Delivering on the Global partner-
September 2010.
1169-1178.
ship for achieving the Millennium
7.
William E. “How the Millennium
14. Kruk
ME, Rockers
PC, Williams
Development Goals: Millennium
Development Goals are unfair to
EH,
et al. Availability of essential
Development Goal 8. The MDG
Africa.”World
Dev 2009;
37(1):
health services in post-conflict
Gap
Task Force Report. ISBN 978-
26-35.
Liberia. Bull
World Health
Organ
92-1-101172-2.
2010; 88: 527-534.

301
21.
United Nations Children’s Fund
24.
Awoonor-Williams JK, Sory EK,
26.
WHO Geneva. Measles deaths
New
York, 2013. Press Release.
Nyonator FK, Phillips JF, Wang E,
decline, but elimination progress
Committing to Child Survival: A
Schmitt ML. Lessons learned from
stalls in some regions. Accessed 7
Promise Renewed. Leaders invest
scaling up a community-based
July 2013; Available at: http://
in
Africa’s future through renewed
health program in the Upper East
www.who.int/mediacentre/news/
focus on child survival. Addis
Region of Northern Ghana. Glob
notes/2013/measles_20130117/en/.
Ababa 16 Jan 2013. Available at:
Health Sci Pract 2013; 1(1): 117-
27.
World Health Organization. Immu-
http://www.apromiserenewed.org .
133.
nization surveillance, assessment
22.
United Nations New York, 2013.
25.
World Health Organization and
and
monitoring. Vaccine prevent-
The
Millennium Development
UNICEF 2013. Progress on Sanita-
able diseases 2012. Accessed 10
Goals Report 2013: Assessing
tion and Drinking Water, 2013
July 2013; Available at: http://
progress in Africa towards the
Update. ISBN 978 92 4 150539 0.
www.who.int/
Millennium Development Goals.
Available at: http://apps.who.int/
immunization_monitoring/
23.
Federal Republic of Nigeria, 2012.
iris/bitstream/10665/81245/1/978
diseases/en/.
Monitoring the situation of chil-
9241505390_eng.pdf.
dren and women. Multiple Indica-
tor
Cluster Survey 2011 Summary
Report.